Colleen Huber, Boris Borovoy
December 19, 2020.
Completed peer-review and revised, January 18, 2021
Abstract
A pandemic that calls the attention of the public, and action by the medical field, is one that raises the total death rate above that of a typical year or season. The COVID-19 era that began in early 2020 has received continuous and rapt attention in the United States for deaths that have occurred. Has COVID-19 resulted in more deaths (known as “excess deaths”) than would have happened in a typical year? An obstacle to answering that question is that COVID-19 testing is flawed and imprecise, for reasons discussed herein, and it is difficult to distinguish COVID-19 from other respiratory illnesses, due to symptoms and signs that are mostly indistinguishable from the common cold, flu or pneumonia. It is possible that deaths of multiple causes have been ascribed to COVID-19, especially due to new peculiarities in mortality reporting during 2020 discussed herein. Therefore, year-over-year comparison of deaths from all causes is likely the best analysis of available evidence of whether the United States is now confronted by a deadly pandemic. The CDC mortality numbers are as yet unaudited by independent parties. Therefore, we compare numbers of obituaries in 2020 and 2019, which are verifiable reports of deaths of specific, identified individuals. We also examine the earnings statements of the largest medical suppliers in the US, to see if their sales of medical oxygen and other medical equipment prove a pandemic. These data all indicate that there has been no pandemic in the US in 2020.
Background
A pandemic is the prevalent spread of a disease over an entire country or worldwide, and there is often increased mortality for its duration compared to more typical years. Early rises in death rate are a warning of an especially dangerous pandemic. In 2020, it has been widely assumed that COVID-19 is an unusually deadly pandemic.
Understanding the COVID-19 phenomenon has been obstructed by several factors.
COVID-19 is assumed to be caused by a coronavirus that is said to be novel, “SARS-Cov-2.” However, SARS is likely a misnomer, because it is an abbreviation of Severe Acute Respiratory Syndrome. It is not at all clear that a majority or even a significant minority of COVID-19 patients have had acute respiratory distress with this illness. Other factors, such as use of over- pressurized ventilators, have led to acute respiratory distress among COVID-19 patients.
The most confusing aspect of COVID-19 is reliance on a manufacturing technique, now nearly universally re-purposed as a test for the presence of the SARS-Cov-2 virus, although there are many problems with this “test.” We list these problems below:
1. The very questionable applicability of the manufacturing technique, the reverse- transcriptase / polymerase chain reaction technique for propagating RNA, now used throughout the world as a test for presence of the particular infectious agent in question, or of other coronaviruses, virions and virus particles that may resemble or share common nucleic acid sequences with the SARS-Cov-2 infectious agent, without distinction among those; and
2. The 80% and higher false positive rate of this “test” in the diagnosis of COVID-19, partially due to cross-immunity to fragments of other coronaviruses, inevitably present in the human body, 1 2 followed by political pressure to recant these findings; and
3. The arbitrary number of iterations of this “test” (cycle thresholds) that must be selected to produce a positive “result”; and
4. Instructions given to physicians by the CDC to code cases as COVID-19 deaths including presumptively, even though multiple severe co-morbidities are typical among individuals whose deaths were called COVID-19;3 and
5. Controversy regarding higher Medicare and private insurance reimbursement for COVID-19 patients than for flu patients,4 5 which may have skewed reported cause of death on death certificates; and
6. Generous financial rewards to hospitals by the US CARES Act for the number of COVID- 19 patients they treat; and
7. The possibility that there may be political influences in altering the true number of deaths from COVID-19.
Two of these problems in particular merit greater attention.
COVID-19 has been very heavily marketed as a pandemic to the US public, with two important aspects that led to false reporting of US mortality data for COVID-19.
The incentive for mis-stated US mortality data is the financial influence created by the US CARES Act, which budgeted $175 billion dollars for distribution to hospitals for treatment of COVID-19 patients, with many hospitals receiving millions of dollars in such aid.6 Specific financial incentives that favored COVID-19 diagnosis over other similar diagnoses such as flu, pneumonia and bronchitis especially, included a Medicare incentive of only $5,000 per patient for pneumonia, but $13,000 per patient for the pathologically indistinguishable COVID-19 pneumonia.7 8 Further, the CARES Act incentive of $39,000 to treat such a patient with a ventilator resulted in financially lucrative outcomes for hospitals, but medically lethal outcomes for patients.9
The core of public confusion and fear of COVID-19 stems from the testing itself. Reverse- transcriptase, polymerase chain reaction (RT-PCR) is a manufacturing technique for producing more RNA nucleic acid sequences. It was not intended by its inventor, the late Kary Mullis, PhD, as a test for an infectious disease. He warned against its use in such an application. He especially warned that it could be misused if the cycles, or iterations, of this procedure were processed too many times on a particular specimen. Regarding the use of RT-PCR to attempt to detect infectious disease, he said, at 35 or 40 cycles, “you can find almost anything in anybody.”10 The CDC acknowledges that 33 cycles or more are unlikely to detect active virus.11 The number of cycles used in “COVID-19 testing” in the US have been above 37, and often well into the 40’s for all of 2020.12 13 Laboratories in the US do not disclose the cycle thresholds that they use in running RT-PCR SARS-CoV-2 tests, except in Florida where the disclosure is mandatory.14 No standardization for cycle threshold values exists across different tests and different laboratories.15
Infectivity was found to be significantly reduced from positive tests when cycles were greater than 24, and that for every 1-unit increase in cycle threshold, the odds ratio of infectivity decreased by 32%.16 Researchers concluded that PCR sensitivity is excellent (can find viral particles very easily), but that its specificity for detecting replicative (active) virus is poor,17 as Dr. Mullis had warned. Nevertheless, RT-PCR has become “the COVID-19 test” used ubiquitously throughout the US and many other countries.
The magnitude of deception resulting from this misuse, overuse, over-cycling and over- advertising of PCR as a COVID-19 testing technique, along with frequent exhortations by politicians to “get tested,” can hardly be overstated. This is the core of the problem of the public falsely believing that there is a pandemic, and that its name is COVID-19.
Therefore, in order to attain the truest picture of the impact of the COVID-19 on public health, it would be helpful to look at deaths from all causes, to see if there has been a significant change.
Deaths attributed to COVID-19 are at the oldest ages; yet age distribution of all-cause mortality did not significantly change during weeks of peak reported COVID-19 deaths
Researcher Genevieve Briand PhD hypothesized that the over-counting of COVID-19 death numbers may be due to society’s heavy focus on that topic, which would eclipse awareness or even reporting of more typical causes of death.18
Dr. Briand found that the proportion of total deaths in US by age group did not change from before COVID-19 to after its peak incidence in the US. The CDC has shown throughout 2020 that peak incidence of COVID-19 deaths occurred the weeks ending April 11 and April 18, 2020,19 as shown in this graph:
Graph 1
 Briand’s research showed that for all weeks of 2020 to date, a consistent proportion, among different age groups, of deaths from all causes occurred. Her research was quickly removed from the internet almost as soon as it was posted. The publisher, then censor, was Johns Hopkins University, with known financial ties to World Economic Forum and Bill and Melinda Gates Foundation, each of which has taken an active role in promoting COVID-19 as the catalyst that justifies a New World Order.20 Several concerns regarding over-reporting of COVID-19 data are enumerated above.
Briand’s research showed that for all weeks of 2020 to date, a consistent proportion, among different age groups, of deaths from all causes occurred. Her research was quickly removed from the internet almost as soon as it was posted. The publisher, then censor, was Johns Hopkins University, with known financial ties to World Economic Forum and Bill and Melinda Gates Foundation, each of which has taken an active role in promoting COVID-19 as the catalyst that justifies a New World Order.20 Several concerns regarding over-reporting of COVID-19 data are enumerated above.
Here is the clearest available photo of Dr. Briand’s graph of the age distribution of total deaths from February 1, 2020, which is before COVID-19 affected the US population, before there was even one death from it, through early September 2020.
Graph by Genevieve Briand
 Our updated graph, derived from CDC data through 01/02/202121 of the same analysis is as follows:
Our updated graph, derived from CDC data through 01/02/202121 of the same analysis is as follows:
Graph 2
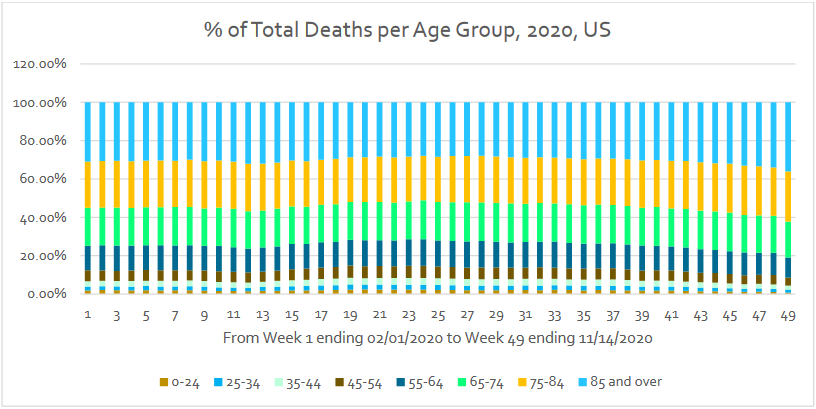 What is especially interesting about the age distribution of total deaths is that there is no extreme change at any time in 2020 of the proportion of total deaths for any age group, except for the last seven weeks, but those weeks do not correspond to COVID-19 peak mortality reporting, which was in April 2020. The CDC showed the weeks ending April 11 and April 18, 2020 (weeks 11 and 12 of the above graph) as the weeks with the highest COVID-19 deaths, yet there is barely perceptible difference in age distribution of deaths, even during those weeks. If there were a pandemic that affected all age groups equally, such a consistency over the year would not be surprising.
What is especially interesting about the age distribution of total deaths is that there is no extreme change at any time in 2020 of the proportion of total deaths for any age group, except for the last seven weeks, but those weeks do not correspond to COVID-19 peak mortality reporting, which was in April 2020. The CDC showed the weeks ending April 11 and April 18, 2020 (weeks 11 and 12 of the above graph) as the weeks with the highest COVID-19 deaths, yet there is barely perceptible difference in age distribution of deaths, even during those weeks. If there were a pandemic that affected all age groups equally, such a consistency over the year would not be surprising.
However, COVID-19 is a peculiar phenomenon in that the average age of death for COVID-19 is beyond the average age of total deaths. Unfortunately, regarding COVID-19, much of the important data still remains hidden. The BBC reports average age of death in Scotland is 79.1, but the average age of COVID-19 death in Scotland is 81.5.22 The mean age of COVID-19 death in France is 79 years.23 If there were a large number of deaths from COVID-19, with average age of death of 79 to 81, there would have been wide swings in age distribution toward the higher age groups during peak time periods of deaths that were attributed to COVID-19. In comparison with the first four weeks studied (February 2020), when there were no COVID-19 deaths, there would have been a rise in the proportion of those in the highest age categories of all deaths. However, that change did not happen. As Briand concluded, COVID-19 had no effect on the percentage of deaths of older people as a portion of the whole population.
The graph below, from Science,24 shows the Infection Fatality Rate of COVID-19. We see that the deaths are skewed strongly toward the upper ages.
 The average life expectancy in the US is 78.7 to 78.9 years.25 26 If the average age of death from COVID-19 is above the average US life expectancy, then COVID-19 cannot be a major independent cause of death, as in cutting short the lives of people who were expected to live longer. This of course varies with individuals, but cannot vary with respect to the population as a whole.
The average life expectancy in the US is 78.7 to 78.9 years.25 26 If the average age of death from COVID-19 is above the average US life expectancy, then COVID-19 cannot be a major independent cause of death, as in cutting short the lives of people who were expected to live longer. This of course varies with individuals, but cannot vary with respect to the population as a whole.
Even from unaudited CDC data so far, it appears that COVID-19 has not made appreciable impact on the overall US death rate. From 2017 through 2020 the rate of deaths in the US population has stayed at 0.9%, keeping pace with population growth, as the following table shows.27

Obituary data
To understand the discrepancy between the announcement of a pandemic that affects almost entirely the elderly, yet does not change the deceased elderly as a proportion of the total deceased, we must look beyond this particular set of data.
The CDC has presented on faith their enumerated death counts. One might ask, but where is the evidence underlying these numbers? Of the largest obituary reporting services in the US, the largest of these with the most transparent data seems to be United States Obituary Notices (USObit.com.) This obituary reporting service reports the deaths of specific, verifiable deceased individuals. The total numbers of deceased reported by USOBit.com are approximately 20% to 25% of total deaths in the US as reported by the CDC. The data shown on their site for 2019 and 2020 is summarized as follows.
Table 1
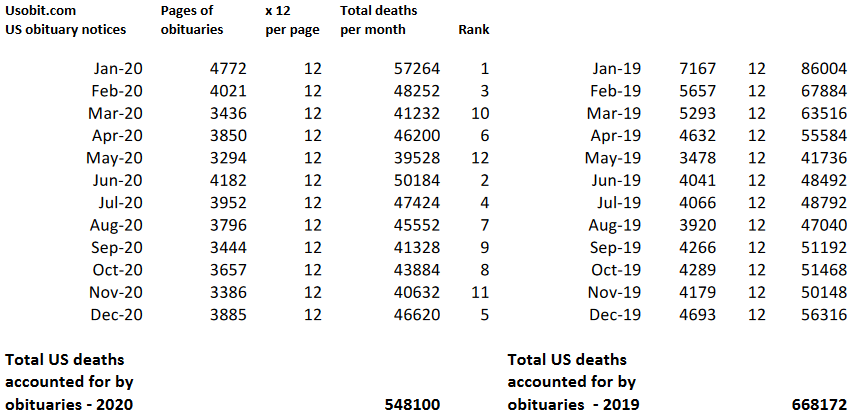 Obituaries of real, identifiable deceased individuals declined by almost 18% from 2019 to 2020. If these obituaries are representative of deaths in the US as a whole, then it is impossible for there to be a pandemic in the United States in 2020. These deaths are at least verifiable, unlike the unaudited, unverified numbers that the CDC presents. It is also interesting that the month with the largest number of COVID-19 deaths according to the CDC, April 2020, ranks 6th out of the 12 months of 2020 regarding total obituaries. Other large obituary services did not respond to requests for information or refused to share information on total numbers of obituaries in 2019 and in 2020.
Obituaries of real, identifiable deceased individuals declined by almost 18% from 2019 to 2020. If these obituaries are representative of deaths in the US as a whole, then it is impossible for there to be a pandemic in the United States in 2020. These deaths are at least verifiable, unlike the unaudited, unverified numbers that the CDC presents. It is also interesting that the month with the largest number of COVID-19 deaths according to the CDC, April 2020, ranks 6th out of the 12 months of 2020 regarding total obituaries. Other large obituary services did not respond to requests for information or refused to share information on total numbers of obituaries in 2019 and in 2020.
Wall Street vs the pandemic story
There are other data that suggest that there is no pandemic, at least not involving a pathogen that causes acute respiratory distress.
We looked at companies that produce and distribute medical oxygen. The following graph shows total sales over the largest of those companies actually declined from 2019 to 2020.
Table 2
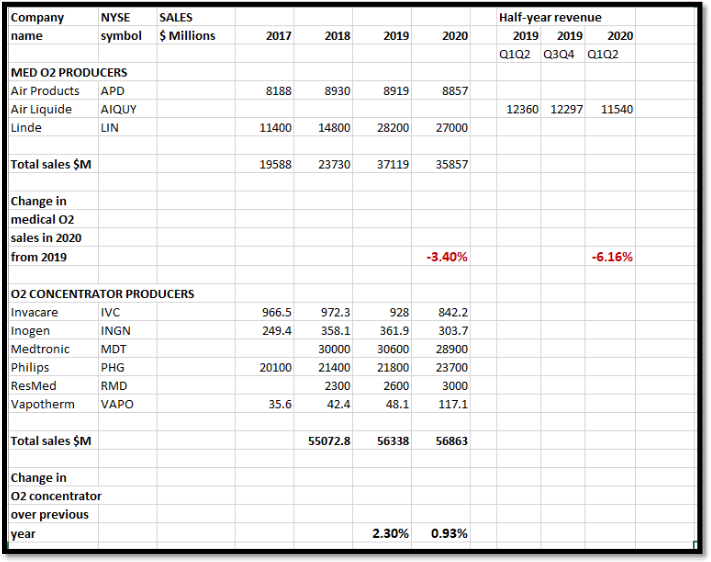 At the beginning of 2020, COVID-19 had no perceptible impact on any aspect of life or business in the US. By the end of 2020, almost every facet of American life had been shaken by the phenomenon of the response to SARS-CoV-2. That is, every aspect except the public’s need for medical oxygen. For the alleged “Severe Acute Respiratory Syndrome” for which SARS-CoV-2 was named, US citizens have actually consumed less supplemental medical oxygen in 2020 than in 2019, despite our growing population, thus disproving a 2020 pandemic involving a respiratory pathogenic virus, i.e. the now legendary SARS-CoV-2 and COVID-19.28
At the beginning of 2020, COVID-19 had no perceptible impact on any aspect of life or business in the US. By the end of 2020, almost every facet of American life had been shaken by the phenomenon of the response to SARS-CoV-2. That is, every aspect except the public’s need for medical oxygen. For the alleged “Severe Acute Respiratory Syndrome” for which SARS-CoV-2 was named, US citizens have actually consumed less supplemental medical oxygen in 2020 than in 2019, despite our growing population, thus disproving a 2020 pandemic involving a respiratory pathogenic virus, i.e. the now legendary SARS-CoV-2 and COVID-19.28
In a related market, oxygen concentrators have been recently innovated to include small, portable backpack units for individuals who are ambulatory with long-term chronic conditions requiring supplemental oxygen, which is thought to account for much of the increase in sales in 2019. This welcome innovation greatly increased mobility and convenience for those dependent on supplemental oxygen. But even those sales did not increase as much in 2020 as they had in 2019, and are mostly irrelevant to a virus thought to be as acutely sickening as SARS-CoV-2. Rather, small travel-size backpacks of oxygen concentrators are more suited to ambulatory patients with chronic COPD, pulmonary fibrosis, and other non-emergent lung diseases.
Then we looked at other medical products.
The five largest medical supply companies in the US are: McKesson, Amerisource Bergen, Henry Schein, Cardinal Health and Medline Industries.29 Their sales for 2019 and 2020, from their corporate earnings reports30 are compared below, as well as their change in growth over that time.
Table 3
 Although these five companies’ sales increased in 2020 over 2019, the growth rate for one year has slowed from the 5-year aggregate overall growth rate for these companies. This is even though the US population has steadily increased through those years.
Although these five companies’ sales increased in 2020 over 2019, the growth rate for one year has slowed from the 5-year aggregate overall growth rate for these companies. This is even though the US population has steadily increased through those years.
Conclusion
On examination of diverse data, from CDC mortality data, to obituaries, to Wall Street earnings reports, there are enough indicators that a pandemic involving a Severe Acute Respiratory Syndrome (SARS) virus could not have taken place, at least not in the United States in 2020.