GENE TRANSFER TECHNOLOGY- YOU ARE THE EXPERIMENT
Scientists have long known that the gene-transfer technologies used in both the Pfizer and J & J COVID-19 vaccines were associated with systemic inflammation and the potential for viral DNA to get inserted into the DNA of body cells as well as reproductive cells. Insertion of the viral DNA coding for the spike protein into reproductive cells, such as eggs and sperm, would then be transmitted to your offspring.
While we were repeatedly told that there was no chance these vaccines could alter our DNA, a study from the winter of 2022 showed that the Pfizer vaccine caused human liver cells to copy the vaccine mRNA into DNA and insert it into the person’s DNA. This was not a surprise. Molecular biologists knew that this was likely. Further, they knew that insertion of viral DNA into the DNA of a person’s immune cells would increase their risks for leukemia. However, most stayed silent as large segments of our population were injected with this experimental gene-transfer technology.1
IS THE WIDESPREAD USE OF GENE-THERAPY/TRANSFER TECHNOLOGY SAFE?
“In 1999 18-year-old Jesse Gelsinger died when an experimental gene treatment designed to treat his metabolic liver disease sent his immune system into overdrive. A few years later, in 2003, researchers reported that several people treated for immunodeficiency developed leukemias, an unfortunate result of the virus randomly inserting its cargo into cancer-promoting regions of the genome.”2
WAIT! WHAT??? Gene transfer technologies, such as those used with the COVID-19 vaccines are known to cause severe inflammatory responses and lead to cancer in some people??
YES. In fact, the Mayo Clinic lists the risks associated with gene therapy as follows:3
- Unwanted immune system reaction. Your body’s immune system may see the newly introduced vaccine particles or the protein they produce as intruders and attack them. This may cause inflammation and, in severe cases, organ failure.
- Targeting the wrong cells. Because this technology can affect more than one type of cell, it’s possible that healthy cells may be damaged, causing other illness or diseases, such as cancer.
- Infection caused by the virus. It’s possible that once introduced into the body, the adenoviral vectors (such as J & J and Astra-Zeneca) may recover their original ability to cause disease.
- Possibility of causing a tumor. If the new genes get inserted in the wrong spot in your DNA, there is a chance that the insertion might lead to tumor formation.
In a recent meeting with AFLDS National State Leaders, Dr. Dana Granberg-Nill asked Dr. Christina Parks about the effects of the spike proteins in the COVID jabs. “When I think of the injuries caused by the spike proteins, I think it is inflammation-driven. Whether it’s the heart, whether it’s the nerves, whether it’s the skin, that that spike protein is causing an inflammation and sometimes and autoimmune response. Have you seen anything along the lines of soft tissue injuries or even bone fractures that are out of proportion to injury in kids?”
Dr. Parks agreed with Dr. Granberg-Nill that there is inflammation but points out there are many more mechanisms than inflammation at work. “When anything gets dysregulated, it causes inflammation,” Parks comments, “The adrenal and T-cell effects are somewhat driven by inflammation but they’re somewhat driven by some really core level dysregulations, not just inflammation. There’s evidence that it may bind major tumor suppressors. It allows huge DNA damage and possibly the formation of cancer cells.”
Parks recognized an earlier study on infants this highlights core dysregulation. “Remember we have that data in infants where when the mother had COVID or was vaccinated, when they were vaccinated it was way worse, but they had literally NO STEM CELLS, almost NONE. So, that’s not just inflammation. That’s a core dysregulation. It could be caused by some event where the cells blow up because of inflammation, but it is not just a standard form of inflammation. There is a lot more going on here.” Parks goes on to explain that our Toll-Like Receptors are down regulated. “That is not inflammation. That is immune suppression. That’s AIDS. So, you’ve got inflammation in conjunction with an autoimmune deficiency. What’s happening is our T-cells are going anergic because of the chronic immune activation. Remember the spike protein keeps getting taken to our lymph nodes, where it keeps being presented, where it keeps causing activation of our T-cells. Eventually, your body tells itself to stand down because you just can’t keep attacking yourself. The T-cells become anergic. If you keep stimulating them after they stand down and are anergic, you’ve got AIDS (autoimmune deficiency). Then, those T-cells actually signal the production of aberrant antibodies. They start signaling the production of auto-antibodies. There is a fair amount of research on that previously, with conditions like lupus.” Dr. Parks believes that is exactly what is happening here. “Remember when your T-cells go anergic, you are NOT protecting the body against infection. Your T-cells are not working, and they are NOT surveilling for cancer.”
“So, you’ve got the disruption of p53’s (a major tumor-suppressor) at the same time your T-cells aren’t working to go around and kill the cancer cells AND the mRNA is going to get inserted into your stem cells. It’s going to get inserted into your DNA. It’s going to cause issues favorable for cancer. If your T-cells aren’t surveilling and killing those cancer cells, the likelihood of leukemias, lymphomas, and other cancers is just going to skyrocket. So, we’ve got really a perfect storm here.”4
IS THE WIDESPREAD USE OF GENE-THERAPY/TRANSFER TECHNOLOGY ETHICAL?
These “gene-transfer” vaccines were designed to force the cells of your body to make as much foreign, viral protein as they can for as long as possible.
The question we should all be asking is, “why would scientists decide to force the body to produce a toxic, foreign viral protein when they knew this would cause the body to attack the cells producing it, as they would be seen by the body as ‘foreign’ invaders?”
The purpose of gene-therapy is to replace the function of a non-functional (mutated) protein with a functional one. Originally, scientists thought they would try to insert the correct gene, coding for the functional protein, into the DNA of each cell. However, if the gene got inserted in the wrong spot, it could cause mutations leading to cancer.
In a cell, your DNA is copied to mRNA, which is then made into a protein. Thus, scientists decided it would be safer and more effective to deliver mRNA that would then be made into a functional protein in each cell. However, the amount of a nano-lipid particles (or adenoviral vectors) that was needed to get enough mRNA into enough cells to effectively replace the function of the defective protein often caused an extreme anaphylactic (or inflammatory reaction), as in the case of Jesse Gelsinger, mentioned earlier. This may be one reason that this technology has been largely abandoned for use in gene therapy and is now being applied to gene-transfer technology in the creation of biologics that are improperly being referred to as “vaccines.” The term “gene-transfer” is being used here because transferring mRNA that forces cells to produce a toxic, foreign viral protein in no way constitutes “therapy.”
Pfizer, J & J and Astra-Zeneca all use gene-transfer technology that transfers the genetic code for the spike protein into the cells of the body. The alarming problem with applying this technology to vaccinology is that the protein that is produced is foreign. Thus, production of the protein by the body’s cells will illicit an ongoing immune response as the body tries to destroy what it sees as a foreign invader, but is really its own cells producing the foreign spike protein.
Secondarily, the spike protein, which the body is being forced to produce, is toxic. It is responsible for most of the health destroying effects of COVID.
What regulatory oversight board approved such an astonishingly bad idea? Who is policing this insanity? It’s time to demand an answer to this question and hold those responsible for foisting this crime on humanity accountable.
To effectively answer these questions, it’s important to understand exactly what gene therapy (gene transfer) technology is and to understand the history of its regulation up to the present day.
WHERE IS THE OVERSIGHT?
So, again, the questions that we must demand answers to are “who were the scientists who were charged with regulatory oversight of this process? What were the standards they used to make their decision?”
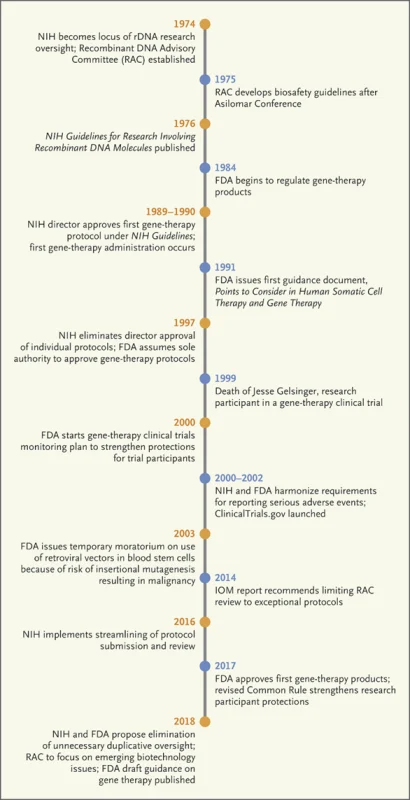
In 1974, the public had expressed concerns over the safety of manipulating genetic material. The idea was offensive to many. The National Institute of Health (NIH) established the Recombinant DNA Advisory Committee (RAC). The RAC issued recommendations to the NIH director through the NIH Office of Biotechnology (OBA). The OBA kept watch over the recombinant DNA research.5
Just a year after inception of the RAC, they issued biosafety guidelines. The guidelines were published in 1976.
In 1984, the FDA began to be involved as they were regulating gene therapy products.
In 1997, the FDA assumed sole responsibility and authority to approve gene-therapy products. The joint NIH-FDA proposal eliminated RAC review and reporting requirements. This reduced oversight. The procedural change altered the regulatory pathway for gene therapy approval.
In the 1990’s many questions arose regarding the safety and efficacy of gene therapy. These concerns came to the forefront in 1999 when Jesse Gelsinger died of a massive immune response during a safety trial of gene therapy.6
The NIH and FDA responded to Geslinger’s death by forming Genetic Modification Clinical Research Information System (GeMCRIS). This database was supposed to provide public transparency in tracking adverse events to gene-therapy products.7
However, in August of 2018, the announcement was made that gene therapies no longer need to be reviewed before clinical studies by begin.8 Then FDA Director, Scott Gottlieb, and NIH director Francis Collins published a paper saying, “There is no longer sufficient evidence to claims that the risks of gene therapy are entirely unique and unpredictable-or that the field still requires special oversight that fall outside our existing framework for ensuring safety.” The idea that gene therapy would continue without oversight should be concerning to every human.9
With that proclamation, the Recombinant Advisory Committee (RAC) and GeMCRIS were summarily dissolved.10
Scott Gottlieb was an advisor to the Trump campaign in 2016, prior to being appointed as the Director of the FDA from 2017 to 2019. During which time he spearheaded approval of the first gene therapy in the U.S., a treatment called Kymriah, which is involved in the treatment of cancer.
It should be noted that this gene therapy differs significantly from the gene transfer technology used in the COVID vaccines in that specific immune cells were isolated and taken out of the body, modified (using gene therapy), and then put back into the body to target cancer cells.
This highly targeted form of gene therapy resulted in such a strong inflammatory response that it carried a boxed warning for Cytokine Release Syndrome (CRS). To deal with this runaway inflammation, a monoclonal antibody that binds to and inactivates the inflammatory cytokine Interleukin-6 (tocilizumab/Actemra) was released alongside it.11
Following his “win” in getting the FDA to finally approve gene therapy technology, Scott Gottlieb moved to the Board of Directors of Pfizer. He made this move immediately prior to the pandemic in late 2019, where he played a role in overseeing the largest clinical trial of gene transfer technology ever seen–the roll-out of the Pfizer vaccine against COVID-19.
 12
12
Largescale acceptance of gene-transfer technology is likely an important goal of both the FDA and pharmaceutical companies as there are currently more than 700 active investigational new drug applications for gene therapies currently waiting for FDA approval.
The number of gene therapy drugs waiting to be approved makes it more urgent that we understand what the oversight process currently is for these products.
All institutions that conduct experimental gene therapy must have oversight from an Institutional Biosafety Committee (IBC).13
Did COVID-19 vaccines undergo this type of oversight, or were they exempted from testing due to being classified as a “vaccine?” This information needs to be made public immediately.
Gene therapy technologies are supposed to be extensively tested for
- Whether they cause a hyper-inflammatory response
- Whether they stimulate the immune system to attack cells making the new protein
- Their effects on fertility
- Whether the viral DNA inserts into the person’s DNA
- Whether viral DNA inserts into the DNA of the person’s eggs or sperm
- Whether the treatment results in the promotion of cancer
How the body handles and excretes the nano-lipid particles/adenoviral vector as well as the protein that is produced is also supposed to be extensively tested.
Where these experiments done? What was found?
If the COVID-19 vaccines were not subject to the normal regulatory oversight process, why not?
Would our government, in conjunction with Pfizer, Moderna and J & J, really use semantics (calling them “vaccines” rather than gene therapy technology) as a way to bypass critical safety reviews??
Pfizer, Moderna, J & J, the NIH and the FDA need to answer these questions.
The American public and all of humanity need to know the answers!
**Source: Gene Transfer Technology- You are the Experiment | America’s Frontline Doctors