PCR: A DNA test becomes a instrument for manipulation
After we have shown in our previous article that the PCR test is not validated (1), we will take the last breath of the PCR test in this article. We show that the PCR test, even if validated, is not able to detect a virus. The PCR test is one of several pillars that all collapse like a house of cards if you look closer. A further finding is the fact that so far no scientific publication has complied with Koch’s postulates on SARS-CoV-2 (gold standard for the detection of a pathogen), which alone means that there is no evidence of a pandemic. Nevertheless, I would like to explain to you in more detail why this PCR test is nothing more than a manipulation tool, because already at this point we can nip this plan-demic in the bud. (2)
The PCR test is not binary!
An important information is that the PCR test is not a binary test, it is not comparable to a pregnancy test that tells you whether you are pregnant or not. So it does not give a clear yes/no result! What they do is, they take a kind of continuum and arbitrarily say that this point is the difference between positive and negative.
The PCR is a production technique!
The polymerase chain reaction (PCR) amplifies a DNA section contained in a sample, i.e. a part of the DNA sequence. Since the SARS-CoV-2 virus does not have any DNA – it is a so-called RNA virus – the RNA is converted into a DNA via an upstream step (reverse transcription/RT). The SARS-CoV-2 test is therefore an RT-PCR test. One starts with one molecule. You start with a small amount of DNA, and every cycle the amount doubles, which doesn’t sound like much, but if you double it 30 times, you get about a billion times more material than at the beginning. So as a manufacturing technique it’s great. What they do is they attach a fluorescent molecule to the RNA as they are making it. They emit a light with one wavelength and you get a response, you get light back with another wavelength. So they measure the amount of light that comes back and that is their surrogate (replacement maker) for how much DNA is present.
To use the PCR as a test, they assume that they start with an unknown number of strands and end with an exponential multiple after n cycles. The initial quantity can be estimated from the quantity of material in scheduling. A major problem is that, since the PCR is an exponential (doubling) process, the errors also grow exponentially. In short, starting from one strand of DNA, the strand is split (divided into two parts) and then complementary strands can grow, the same process that occurs in a cell during mitosis (cell division).
The set cycles decide on a positive or negative result
Unfortunately, there is no calibration for the PCR test, not only are there different PCR tests that are set for different sequence sections of the claimed SARS-CoV-2, but also each laboratory can set an arbitrary cut-off (threshold). And here it gets wild!
“In one paper,” “I found 37 cycles as a cut-off” Young BE et al. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore. JAMA. 2020 Mar 3. (3)
If you did not get enough fluorescence (4) in 37 cycles, you are considered negative. If the fluorescence was obtained under 37 cycles, you will be considered positive.
In another paper the cut-off was 36 cycles. 37 to 40 were considered “undetermined”. This means that if within 36 cycles sufficient fluorescence, virtually enough material was doubled, one was considered positive, while over 40 cycles were considered negative. If indeterminate, further tests were performed. Li Q. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med. 2020 Jan 29. (5)
It is therefore quite possible that different hospitals, different states, Canada vs. the USA, Italy vs. France all use different cutoff sensitivity standards of the Covid test. So if you cut off at 20 cycles, they would all be negative. If you score at 50, maybe they’re all positive. At 36 cycles, you’ve already doubled the material to almost 70 billion.
Excerpt from an interview with David Crowe: “I think if a country said, ‘You know, we have to stop this epidemic,’ they could quietly send around a memo saying, ‘We shouldn’t set the cut-off at 37 cycles, if we set it at 32, the number of positive tests drops dramatically. If that’s still not enough, they could set it at 30 or 28 cycles or something like that. That way you can control the sensitivity.” (6)
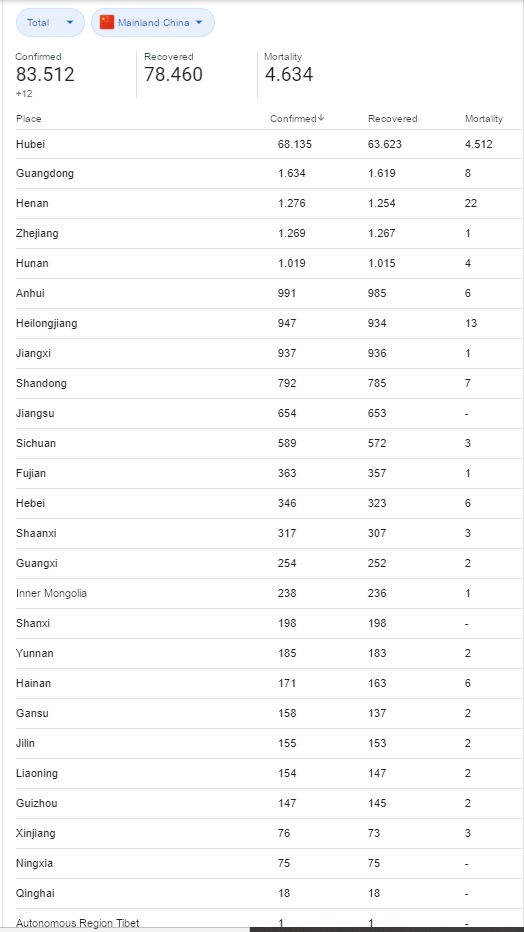
Yes, you read that correctly. Labs can manipulate how many “cases” of Covid-19 your country has. Is that how the Chinese made their case load suddenly disappear?
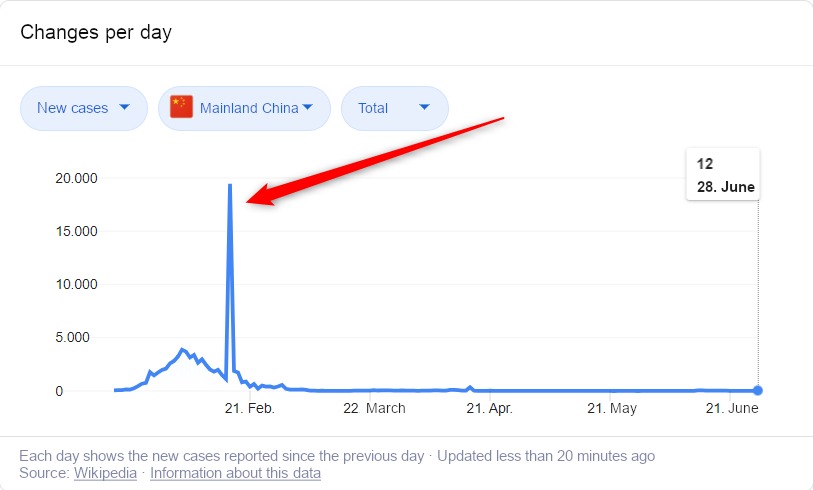
Note: Outside of Wuhan, only 122 people died in all of China with a positive PCR test or no test at all, but even less accurate a lung CT, which was used as a surrogate. This is as crazy as it is incredible.

So you see, with one PCR test, a government can summon anything, as well as stop it from one day to the next. The trust in the PCR test to use it as a virus detection was questioned from the beginning of his invention by the inventor Kary B. Mullis, who even called this practice “oxymoron”, a contradiction in terms (see below).
Patients jumped from a positive result to a negative result and vice versa
Another reason why we know this is fake is a remarkable set of graphics published in JAMA by some people from Singapore. (7) These diagrams were published in the Supplemental Information, which indicates that no one should read them. EFigure 3A page 6. (8)
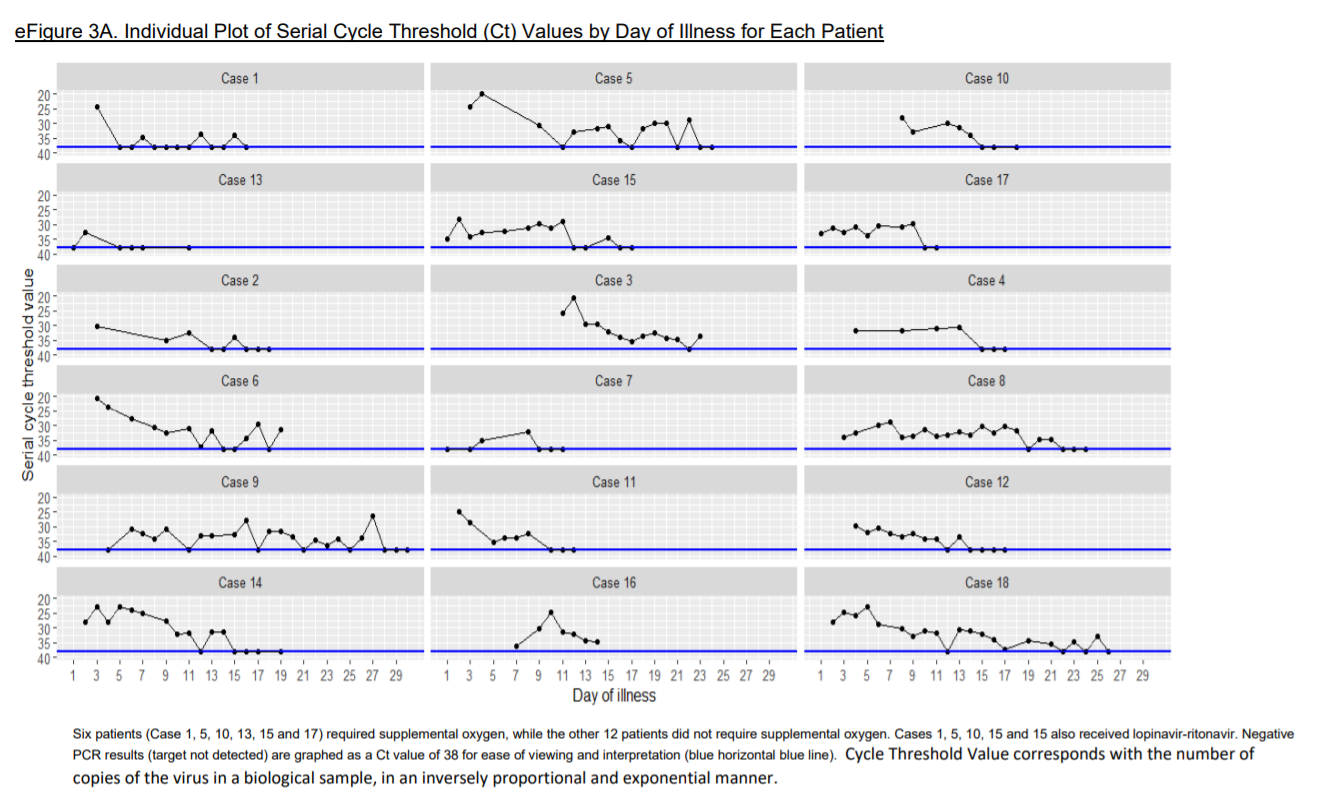
So there were 18 diagrams of 18 different people. And in this hospital in Singapore they did daily coronavirus tests and they recorded the number of PCR cycles required to de-tect fluorescence. Or if they could not detect the fluorescence after…37 cycles, they put a dot at the bottom of the chart, which was considered a negative result. So in this group of 18 people, the majority of people went from positive, which is normally read as “infected”, to negative, which is normally read as “not infected”, and back to positive-infected. So how do you interpret this? No matter what you do, even if you set the cut-off to a different number of cycles, it would be an arbitrary division up or down. But there’s no guarantee that if you did that, you wouldn’t still have the same problem. So you cannot solve the problem by changing this arbitrary binary division. So basically, what this means is that the test can’t detect infection. Because if this PCR test could do this, how is it possible that within a hospital with the best anti-infection measures in the world, patients could be tested from positive to negative from one day to the next and so on?
The amount of RNA does not correlate with the disease!
Take another look at the graph of the 18 patients. Theoretically, the PCR cycle number, where DNA is detectable, tells us the relative amount of RNA. No matter what initial amount was necessary to be considered detected in the 20th cycle, in the 21st cycle there would be a cyclical doubling and sensitivity, and in 30 cycles already 1000 times the amount. One could therefore expect that more alleged “virus” debris would be detected in test subjects who are ill, and therefore a smaller number of propagation cycles would be necessary in their PCR test.
This is the reason why the authors have separated the first six diagrams from the remaining twelve. The first six were the people who were sick enough to need oxygen. However, the graph clearly shows that the six sicker people did not have significantly higher amounts of RNA.
An important video that we recommend (for further information) is Corona – An epidemic mass hysteria. (9)
One of the best scientific summaries of the whole corona panic can be found in David Crowe – Flaws in Coronavirus Pandemic Theory (This document is continuously updated). (10)
The PCR test does not search for a complete genome (genome of a living being or a virus)
Each manufacturer of a PCR test decides for himself which RNA sections (parts of the genome) he wants to test for, which are most specific for him. In principle, RT-PCR can detect two different gene sequences (“targets”) for SARS-CoV-2 and, if both sequences are detected in one sample, achieves specificities of almost 100%. The test of the Berlin Charité – Christian Dorsten (11) only knows parts of the claimed pathogenic virus according to “2 (two) genes from the genome of a total of 10 (ten) genes of the corona virus”. So we have several massive problems here.
- We only have a mentally constructed genetic strand of a virus consisting of short gene sequences! (12)
- There is no scientific publication in which Koch’s postulates were adhered to. The Chinese studies even admit this, as an example A Novel Coronavirus from Patients with Pneumonia in China, 2019, where it says literally under the heading Discussion “Although our study does not fulfill Koch’s postulates”.
- It does not search for the complete genome in the PCR, but only for 2 of 10 genes.
- These sections also occur in other claimed “cold viruses”. Drosten himself was the one who said in his podcast (13) that his test also responds to RNA sequences (corona) of cattle and bats. Drosten also said that his test would fail (false positive) if another corona virus (cold virus) RNA sequence was present in humans. (vaccinations).
- Inaccuracies in specificity lead to massive false-positive results. Currently with the latest RKI data 85% false-positive results. Samuel Eckert (14) has provided a fantastic analysis including an Excel list, (15) which includes the search rate. Dr. med. Steffen Rabe (16) has also presented an analysis of the calculation and has also provided a calculator. (17)
- Simply put, imagine the following example: You want to prove that there is a car in the garage, so you look for a feature specific to you, the exterior mirror. If you find this exterior mirror, this is considered proof that the whole car is there. Since this is already more than inaccurate, the question arises as to what this has to do with infectivity. Just because you have found a wing mirror, you are claiming that the car is also present and that there is fuel in the tank to drive!
- Another example: What do 2 (two) genes from the genome of a total of 10 (ten) genes of the corona virus“. Imagine you have 20 screws (RNA sections) for a cabinet (Ikea). The whole cabinet has 100 screws. But the same 20 screws (RNA sections) are also found in a cupboard from another furniture store, as well as in other cupboards. But you have never built the cabinet (virus isolated/pure culture), so you have never seen it in reality. One has put it together in one’s mind (genetic material strand from short gene sequences). As in God’s name one wants to say now with the “alleged” finding of the 20 screws that at the same place of the screws (RNA sections) also the cabinet (complete genome) is to be found. This does not even take into account infectivity.
The WHO allowed an even more imprecise testing method to obtain more positive tests
In a publication of 19.03.2020, the WHO has decreed for regions affected by the pan-demic that in this case, the detection of only one of the targets is sufficient for the sample to be found “positive”: “In areas where COVID-19 virus is widely spread a simple algorithm might be adopted in which, for example, screening by rRT-PCR of a single discriminatory target is considered sufficient”. (18) This naturally results – due to the lack of double determination – in a significantly lower specificity and thus a significantly higher rate of false-positive findings. This generous offer of the WHO was of course accepted by numerous laboratories (fewer determinations means: less costs), the MVZ Augsburg even got an article in an Austrian newspaper Wochenblick (19) via its blog entry of 03.04.20. The entry has been deleted from the laboratory’s blog in the meantime, but was definitely still there on 18.05.20. (20) It is not known how many laboratories issue positive results for the detec-tion of one target, how many determine both targets from the beginning and how many at least positive tests with one target are then checked with the other (retesting as de-scribed in the article of the NZZ below) – due to this double determination or retesting, the specificity is obviously increased relevantly beyond 99.3%.
To which value? Here RKI, PEI & Co are silent… .
A PCR test cannot tell anything about the viral load
22.03.2022: Lothar Hirneise: Question about the PCR test
“Can someone explain to me why you need a PCR test to detect corona? PCR tests multiply the virus BEFORE testing. According to virologists like Drosten, the virus must multiply millions of times before symptoms appear. Then you don’t need a PCR test anymore, you can detect it directly in your blood! Strange, isn’t it?” (21) (22)
This hits it quite well. After everything we have just learned, we know that neither a whole virus (genome) nor the RNA section we are looking for can say anything about infectivity.
I would like to refer to the origins of PCR and recommend the following article from Christine Johnson – Viral load and the PCR. (23)
Kary B. Mullis – The inventor of PCR says it cannot detect a virus
The PCR test cannot detect a virus, as the inventor Kary B. Mullis himself confirmed; (24) he even called this practice “oxymoron” (a contradiction in terms). In order to demand scientific proof, he even met with Prof. Luc Montagnier, the man who, according to official sources, is said to have discovered the HI virus. But he could not provide a single proof. (25). Kary B. Mullis – Why they cannot be used to prove the HIV infection (26)
Karry Mullis: …with PCR if you do it well you can find almost anything in anybody….It doesn’t tell you that you’re sick.
A positive PCR test does not indicate that you are ill
- For example, a guidance document (p. 36) on PCR testing from the US CDC states: “The detection of viral RNA may not indicate the presence of an infectious virus, or that 2019-nCoV is the trigger for clinical symptoms.” (27) That means: A positive test does not guarantee that the COVID virus causes an infection at all. And, uh, if you read between the lines, the COVID virus may not be in the patient’s body.
- The instructions for use for the test SARS-CoV-2 Assay (Panther Fusion®️ System) from Hologic, Inc. 2002-03 are: “Some people become infected but don’t develop any symptoms and don’t feel unwell.” (page 2) (28)
- Creative-Diagnostics Product Information on the Test Kit “SARS-CoV-2 Coronavirus Multiplex RT-qPCR Kit (CD019RT) “This product is for research use only and is not intended for diagnostic use.” Intended use” is indicated as follows: “This product is intended for the detection of the 2019 Novel Coronavirus (2019-nCoV). The result of detection of this device is for clinical reference only and should not be used as the sole evidence in clinical diagnosis and treatment”. Source of the test kit (29) and following the general source (30) for this.
As long as no isolation (Koch’s postulates) has taken place, the pathogenic virus remains a model
Where does the RNA come from? Is this “foreign” RNA (a “bad” virus) or does it come from something that exists in symbiosis with our body (a “good” virus)? Is it perhaps an expression of a defence/cleaning or healing reaction of our body and therefore to be regarded positively? Is it caused by contamination of the sample at the time of sampling or in the laboratory? Has this RNA perhaps already been “supplied” in the components of the test kits, as happened for example in Great Britain? (31) (These questions are central to the paradigm of virology, namely that viruses exist and in many cases cause disease. What if there are no disease-causing viruses at all. Dr. Stefan Lanka has uncovered some of these in the measles process. He has won this process and not only because of a formal error. You can read a complete summary here. (32)
The belief in a rapid test leads to an epidemic that did not exist
An article in the NY Times – Faith in Quick Test Leads to Epidemic That Wasn’t tells a story about relying on a test that has misled everyone. (33)
“Now, as they look back on the episode, epidemiologists and infectious disease specialists say the problem was that they placed too much faith in a quick and highly sensitive molecular test that led them astray.”
4 out of 5 people who maintain a positive PCR result remain asymptomatic
Up to 80% of all test positive individuals remain symptom-free. (34) Even among 70-79 year olds, about 60% remain symptom-free. (35) Over 95% of all persons show at most moderate symptoms. (36)
Finally, my tip to you, if you ever get a positive result, request another test immediately, preferably at the reference laboratory. Ask with which test they were tested, the deficits of the different tests can be serious. This is shown in the following ring test: Instand e.V. has found a sensitivity of 99% and a specificity of 92.4 – 98.6% in the most recent so-called round robin tests for RT-PCR.
Instand Society for the Promotion of Quality Assurance in Medical Laboratories e.V. –
Commentary on the Extra- EQAS 340, published on 02.05.2020 (37)
Here you can find the link to the document of the interlaboratory comparison. (38)
Absence of a valid gold standard
This is a fundamental point. Tests need to be evaluated to determine their accuracy – more precisely their “sensitivity” and “specificity” (39) – by comparison with a “gold standard”, which means the most accurate method available. As an example of a pregnancy test, the gold standard would be pregnancy itself. But as the Australian infectious disease specialist, Sanjaya Senanayake, for example in an ABC TV interview in an answer to the question “How accurate is the [COVID-19] test? He explained: “If we had a new test to detect [the bacterium] staphylococci in the blood, we would already have blood cultures, which is our gold standard that we have been using for decades, and we could compare this new test to that. But for COVID-19 we don’t have a gold standard test.” (40) ——– Jessica C. Watson of Bristol University confirms this. In her recent article “Interpreting a covid-19 test result” published in the British Medical Journal, she writes that there is “no gold standard “for COVID-19 testing that is so clear”. (41) But instead of classifying the tests as unsuitable for SARS-CoV-2 detection and COVID-19 diagnosis, or pointing out that only a virus detected by isolation and purification (Koch’s postulates) can be a solid gold standard, Watson seriously asserts this The “pragmatic” COVID-19 diagnosis itself, especially the PCR tests themselves, “is possibly the best available” gold standard “. However, this is not scientifically based. Apart from the fact that it is downright absurd to use the PCR test itself as part of the gold standard for evaluating the PCR test, there are no particular symptoms for COVID-19, as even people like Thomas Löscher, former head of the The Department of Infection and Tropical Medicine at the University of Munich and member of the Federal Association of German Internists has conceded. (42) And if there are no particular symptoms for COVID-19, the COVID-19 diagnosis – contrary to Watson’s statement – cannot serve as a valid gold standard. Moreover, “experts” like Watson overlook the fact that only virus isolation, i.e. a clear virus detection, can be the gold standard.
Using a PCR test to detect a virus is like trying to tell if someone has bad breath by looking at their fingerprint.
We have also contacted Dr. Charles Calisher, who is an experienced virologist. In 2001, Science published a “passionate plea … to the younger generation” by several experienced virologists, including Calisher, and said “[Modern virus detection methods such as] smooth polymerase chain reaction […] say little or nothing about how a virus reproduces, what animals carry it, [or] how it makes people sick. It’s like trying to tell if someone has bad breath by looking at their fingerprint.” (43)
Translated & reblogged Version – Original here
Telegraph main page with overview of all articles: Link
Visit our Telegram Channel for additional news & information: Link
Chat with like-minded in our Telegram Chat Group: Link
Please support to keep this blog alive: paypal
References:
(1) The PCR test is not validated
(2) We ran a massive viral pandemic simulation. Here’s what we learned about managing Coronavirus.
(3) Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore
(4) Fluorescence entry on Wikipedia
(5) Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia
(6) Was the COVID-19 Test Meant to Detect a Virus?
(7) Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore
(8) Epidemiolgic features and clinical course of patients infected with SARS-CoV-2 in Singapore. Supplementary Online Content
(9) Corona – An epidemic mass hysteria. – GERMAN ONLY
(10) Flaws in Coronavirus Pandemic Theory
(11) Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR
(12) Misinterpretation of a virus
(13) Coronavirus update: Need abbreviations for vaccine approval
(14) DROSTEN und das RKI WIDERLEGT! Die WAHRHEIT über die PCR Tests! Sind die Maßnahmen noch haltbar? – GERMAN ONLY
(15) Excel Calculator by Samuel Eckert
(16) The more tests, the less basic rights… Statistics for advanced users
(17) Excel calculator by Dr. med Steffen Rabe
(18) Laboratory testing for coronavirus disease (COVID-19) in suspected human cases
(19) WHO recommended completely non-specific corona virus tests
(20) Changed diagnostic layout of SARS-CoV2 PCR results
(21) webpage from Lothar Hirnreise
(22) Facebook Post Lothar Hirnreise
(23) Viral Load and the PCR
(24) Has Provincetown become protease town?
(25) Why I Began Questioning HIV (From the House of Numbers Deluxe Edition DVD
(26) see 23
(27) CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel
(28) SARS-CoV-2 Assay (Panther Fusion® System)
(29) SARS-CoV-2 Coronavirus Multiplex RT-qPCR Kit (CD019RT)
(30) SARS-CoV-2 Coronavirus Multiplex RT-qPCR Kit
(31) Coronavirus testing effort hampered by kits contaminated with Covid-19
(32) The Federal Court of Justice destroys the belief in Viruses
(33) Faith in Quick Test Leads to Epidemic That Wasn’t
(34) Covid-19: four fifths of cases are asymptomatic, China figures indicate
(35) Field Briefing: Diamond Princess COVID-19 Cases
(36) Studies on Covid-19 lethality
(37) Service for EQA tests
(38) Report on Extra External Quality Assessment Scheme Group No. 340 Virus Genome Detection – SARS-CoV-2
(39) COVID19 PCR Tests are Scientifically Meaningless
(40) ABC TV interview Australian infectious disease specialist Sanjaya Senanayake
(41) Interpreting a covid-19 test result
(42) see 39
(43) see 39
Article Source: https://telegra.ph/PCR-A-DNA-test-becomes-a-instrument-for-manipulation-08-02