STORY AT-A-GLANCE
- By May 2020, it had become apparent that the standard practice of putting COVID-19 patients on mechanical ventilation with ventilators was a death sentence
- Between 50% and 86% of COVID patients placed on life support ended up dying
- By May 2020, doctors had also found that high-flow nasal cannulas and proning led to better outcomes than ventilators
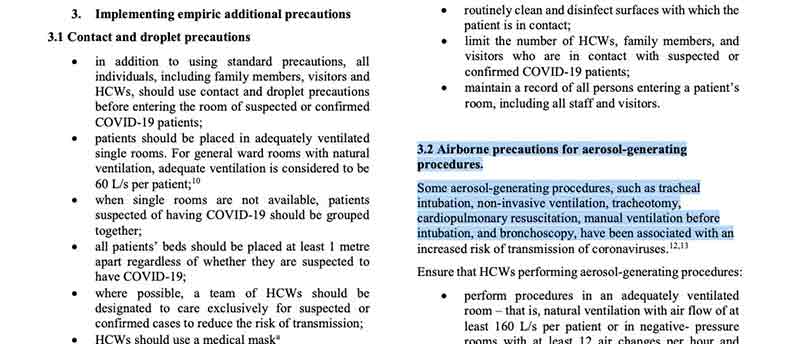
- The World Health Organization promoted the use of ventilators as a way to purportedly curtail the spread of virus-laden aerosols, thereby protecting other patients and hospital staff. In other words, suspected COVID patients were sacrificed to “protect” others
- The matter becomes even more perverse when you consider the fact that many “COVID cases” were patients who merely tested positive using faulty PCR testing. Hospitals also received massive incentives to diagnose patients with COVID and put them on a vent
By May 2020, it had become apparent that the standard practice of putting COVID-19 patients on mechanical ventilation with ventilators was a death sentence.1 As early as April 9, 2020, Business Insider reported2 that 80% of COVID-19 patients in New York City who were placed on ventilators died, which caused a number of doctors to question their use.
The Associated Press3 also publicized similar reports from China and the U.K. A U.K. report put the figure at 66%, while a small study from Wuhan, China, put the ratio of deaths at 86%. Data presented by attorney Thomas Renz in 2021 showed that in Texas hospitals, 84.9% of patients died after more than 96 hours on a ventilator.4
The lowest figure I’ve seen is 50%.5 So, somewhere between 50% and 86% of all ventilated COVID patients died. Compare that to historical prepandemic ratios, where 30% to 40% of ventilated patients died.
High-Flow Cannulas and Proning Were Always More Effective
Meanwhile, doctors at UChicago Medicine reported6 getting “truly remarkable” results using high-flow nasal cannulas in lieu of ventilators. As noted in a press release:7
“High-flow nasal cannulas, or HFNCs, are non-invasive nasal prongs that sit below the nostrils and blow large volumes of warm, humidified oxygen into the nose and lungs.
A team from UChicago Medicine’s emergency room took 24 COVID-19 patients who were in respiratory distress and gave them HFNCs instead of putting them on ventilators. The patients all fared extremely well, and only one of them required intubation after 10 days …
‘Avoiding intubation is key,’ [UChicago Medicine’s Emergency Department’s medical director Dr. Thomas] Spiegel said. ‘Most of our colleagues around the city are not doing this, but I sure wish other ERs would take a look at this technique closely.'”
The UChicago team also endorsed proning, meaning lying in the face-down position, which automatically improves oxygenation and helps alleviate shortness of breath.
Yet despite these early indications that mechanical ventilation was as unnecessary as it was disastrous, placing COVID patients on life support is standard of care to this day, more than three years later. How could that be?
How China and the WHO Created Ventilator Hysteria
In a September 30, 2020, Substack article,8 journalist Jordan Schachtel described how China and the World Health Organization came up with and nurtured the idea that mechanical ventilation was the correct and necessary first-line response to COVID:
“In early March, when COVID-19 was ravaging western Europe and sounding alarm bells in the United States, the WHO released COVID-19 provider guidance9 documents to healthcare workers.
Citing experience ‘based on current knowledge of the situation in China,’ the WHO recommended mechanical ventilators as an early intervention for treating COVID-19 patients. The guidance recommended10 escalating quickly, if not immediately, to mechanical ventilation.
In doing so, they cited the guidance being presented by Chinese medical journals, which published papers in January and February claiming that ‘Chinese expert consensus’ called for ‘invasive mechanical ventilation’ as the ‘first choice’ for people with moderate to severe respiratory distress.
The WHO further justified this approach by claiming that the less invasive positive air pressure machines could result in the spread of aerosols, potentially infecting health care workers with the virus.”
That last paragraph is perhaps the most shocking reason for why millions of COVID patients were sacrificed. They wanted to isolate the virus inside the mechanical vent machine rather than risk aerosol transmission.
In other words, they put patients to death in order to “save” staff and other, presumably non-COVID, patients. If you missed this news back in 2020, you’re not alone. In the flurry of daily reporting, it escaped many of us. Here’s the description given in the WHO’s guidance document.
Strangely enough, while the U.S. quickly began clamoring for ventilators, China started relying on them less, and instead exported them in huge quantities. As noted by Schachtel, “China was making a fortune off of manufacturing and exporting ventilators (many of which did not work correctly and even killed patients11) around the world.”
Source: How COVID Patients Died for Profit