Deaths continue to run at extraordinary levels in England and Wales. In the week ending January 13th 2023 there were 17,381 deaths, which is 2,837 or 19.5% above the five-year average. This is despite the five-year average having risen due to the early 2021 Covid wave. Compared to the pre-pandemic five-year average of 13,822 it is 3,559 or 25.7% above average.
There were 922 deaths with Covid registered on the death certificate, of which 654 were registered as due to Covid as underlying cause. This leaves 2,183 excess deaths from a different underlying cause. Since the wave of excess non-Covid deaths began in April the total now stands at 34,691.
I have previously noted how waves of excess non-Covid deaths appear to correlate with the Covid booster campaigns in spring and autumn, as seen in the chart below, which shows deaths by date of occurrence in England and Wales.
It’s clear, however, that these correlations with booster rollouts are far from determinative of the overall shape of the curve. In particular, deaths remained high during the summer and have spiked over the winter, despite few boosters being delivered in those periods.
The Health Advisory and Recovery Team (HART) has noted this week that high-level mortality data like these do not contain an “obvious smoking gun” pointing to vaccines causing high numbers of deaths specifically during the vaccination campaigns. Rather, the excess deaths are broadly spread throughout the year. The appearance is of something generally raising the likelihood of death, or equivalently, reducing life expectancy. (This doesn’t appear to be due to an ageing population; see here for a discussion on this point.)
The lack of correlation with vaccination programmes has led some to question the role that vaccines are playing in driving the excess deaths and advance arguments in support of other possible explanations, such as Long Covid, the NHS crisis and the legacy of lockdown including missed treatment. While some of these other contributors may be valid, it would be wrong to rule out a role for the vaccines simply on the basis of a lack of correlation with vaccination campaigns. This is because the mechanisms by which a vaccine may injure a person are not fully understood, and those for which understanding is more developed, such as auto-immune reactions due to the persistence of spike protein in the blood and organs, give plenty of scope for a delayed effect. In particular, we should note that many of the excess deaths are related to the heart and circulatory system, and the vaccines are known to increase the risk of such deaths.
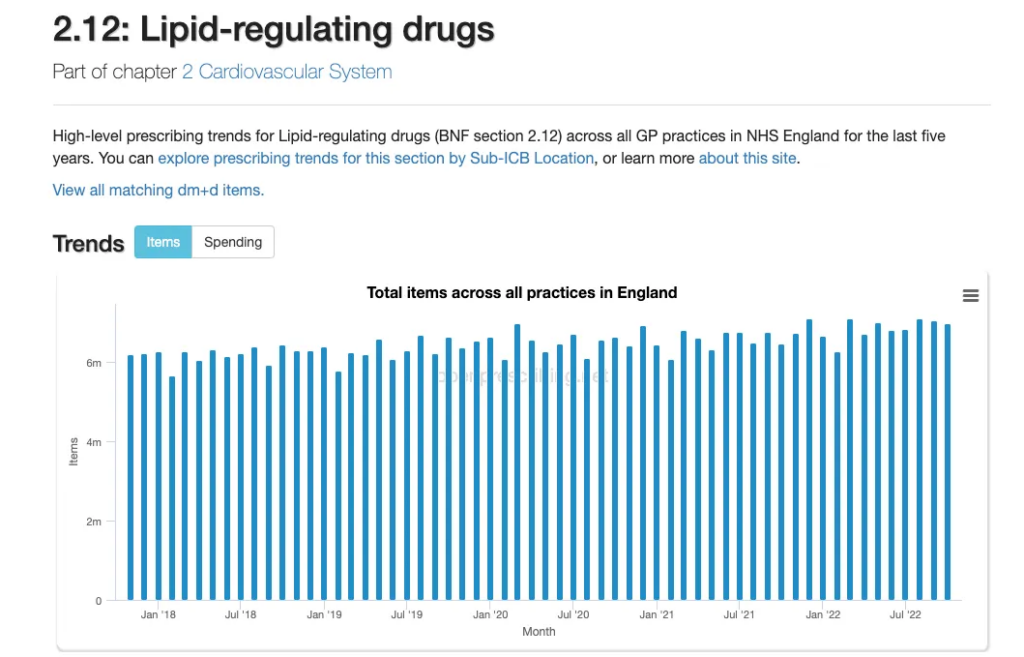
Chief Medical Officer Chris Whitty has recently claimed that 5,170 deaths in men aged 50-64 could have been helped by heart medications that were missed during the pandemic. Health Secretary Steve Barclay agreed, saying that “we know from the data that there are more 50 to 64-year-olds with cardiovascular issues” – a state of affairs he blamed on “the result of delays in that age group seeing a GP because of the pandemic and in some cases, not getting statins for hypertension in time”. The British Heart Foundation published research earlier this month which made similar claims.
However, such claims were dismissed by Dr. Carl Heneghan, Professor of Evidence-based Medicine at Oxford University, and his colleague Dr. Tom Jefferson, who wrote that the extra cardiovascular disease deaths cannot be accounted for by a fall in drug treatment or drop in risk monitoring, “given the lack of evidence of an effect”. In making this assessment they relied in part on a major recent study reviewing the trial data on statins and concluding that the benefits of statins were minimal and most of the trial participants who took statins derived no clinical benefit. Dr. Heneghan and Dr. Jefferson also noted that the claimed reduction in prescriptions appears to be illusory, with rises and falls well within normal levels.
Unlike allegedly missed prescriptions, the NHS crisis is more plausibly contributing to excess deaths, as people experience severe delays getting urgent medical attention. However, the crisis can hardly explain sustained levels of deaths throughout the year or generally increased demand for health services. Something must be making people sicker in the first place.
As I have noted previously, the main alternative explanation is the after-effects of the virus, also known as Long Covid. Interestingly, the British Heart Foundation dismisses this as a factor, laying the blame entirely on access to healthcare – though is there an agenda here of calling for more resources for the sector? But many others see the virus as a much bigger factor than the vaccines in driving additional heart deaths.
One problem for the vaccine-deaths hypothesis, however, is the lack of excess working-age deaths in a number of highly vaccinated countries. Ron Unz has written an article drawing attention to this point, noting that while working-age mortality has been very high in the United States and U.K., some other countries, including highly vaccinated ones, have been exempt from this trend.
To develop his argument, Unz draws on analysis which shows that a very strong predictor of working-age mortality in 2022 is mortality in 2020, as illustrated in the charts below.
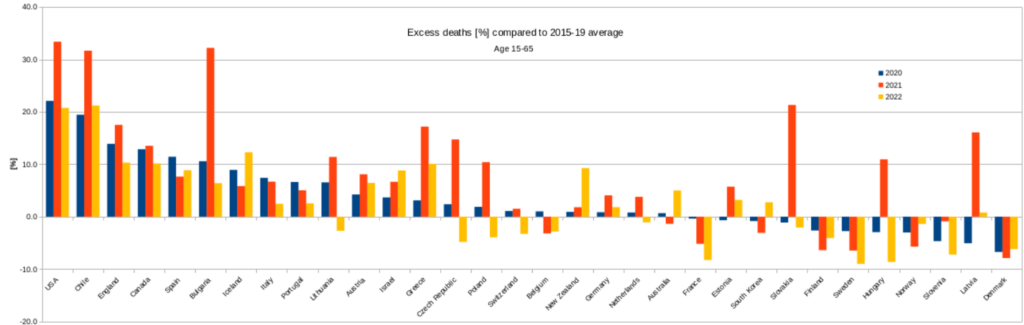
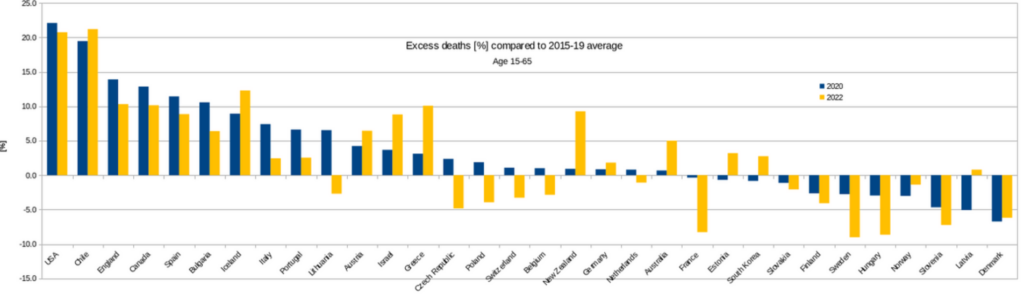
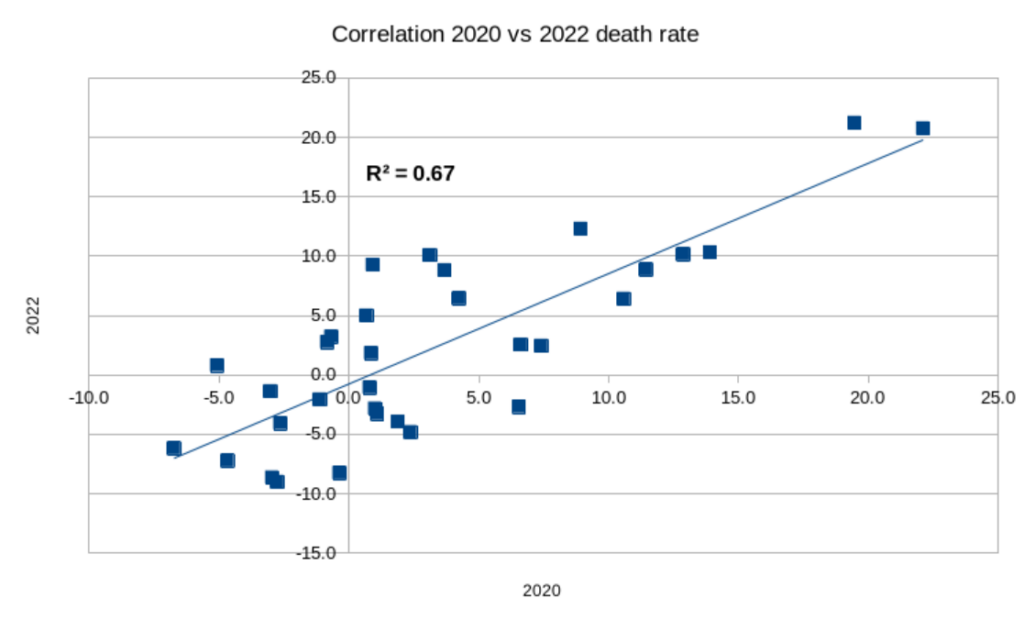
From this Unz concludes that: “The level of 2022 deaths was largely determined by the same factors, probably the interaction of Covid infections with local health characteristics, such as obesity levels and the strength of the public health system rather than having been influenced by the vaxxing.”
This correlation is a very helpful observation, but it actually has the opposite meaning to that which Unz takes from it. Far from suggesting the vaccines are not playing a role, it is consistent with the vaccines playing a significant role. This is because the elevated deaths in 2020 were caused largely by COVID-19 (as well as lockdown measures). But during 2021 and in 2022, Covid was no longer driving excess deaths. Whether this was due to protection from the vaccines, the growth of natural immunity or the arrival of the milder Omicron variants is not relevant here. What matters is that excess deaths shifted from being primarily respiratory related, driven by COVID-19, to being cardiovascular related, driven by an unknown cause.
So, what was now driving these excess deaths, which, as Unz notes, appear to be occurring among the same risk groups as were at risk of serious COVID-19? Unz proposes it is still Covid, and that despite the reduction in the severity of the disease, it is the virus behind the scenes driving the extra cardiovascular deaths.
A critical point here is that this is a false dichotomy: an argument like this for the virus being involved in non-Covid cardiovascular deaths is really also an argument for the vaccines potentially being involved as well. This is because one of the main arguments for the vaccines being involved is that the mRNA and spike protein travel to various organs, especially the heart, and persist there for weeks and months, causing injury and triggering auto-immune attacks – a mechanism supported by a number of autopsy studies. But this is a very similar mechanism to how the virus may contribute to problems with the heart and other organs. Indeed, it is likely that both are contributing to the effect, reinforcing each other in various ways. Another possibility is that the immune tolerance induced by repeated vaccinations is contributing to the persistence of the spike protein in the body. Either way, it means that the underlying risk factors for Covid death will often be the same for vaccine death, and the correspondence between mortality in 2020 and 2022 would therefore be expected.
The question, then, is whether the virus or vaccines are playing the bigger, more fundamental role in driving excess heart deaths.
One reason for thinking that the vaccines may be playing a big part is that the vaccine enters the body via the blood directly whereas the virus enters via the respiratory tract and thus has much more limited access to the blood and heart in most cases.
Further evidence supporting a role for the vaccines comes from the work of Professor Christine Stabell-Benn and colleagues, who looked at the vaccine trial data and found no overall mortality benefit from the mRNA vaccines, and a particular signal for increased heart deaths. This suggests that while the vaccines reduce Covid deaths they may increase other deaths, particularly from cardiovascular causes.
Some health experts in Japan have come to a similar conclusion. In Japan, Covid deaths have actually been increasing after each booster campaign. However, public health authorities have noted that the ‘Covid’ deaths now are more likely to be test-positive deaths from cardiovascular problems rather than classic respiratory deaths. There are also many non-Covid excess deaths in Japan, largely from heart problems.
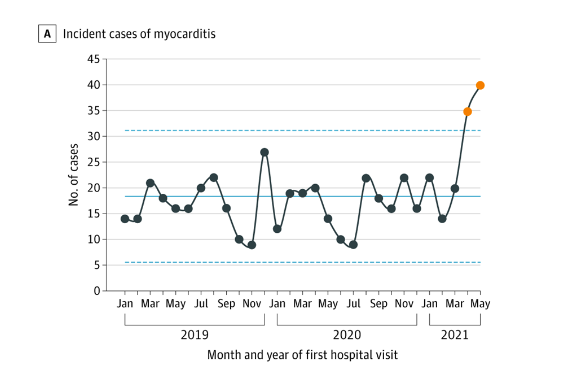
With respect to myocarditis in particular, a recent analysis by HART notes that elevated myocarditis admissions began with the vaccine rollout and did not occur in 2020, indicating a limited role for the virus and a major role for the vaccines.
Given this evidence that the vaccines may be playing a large role in excess deaths, why then are working age deaths below average in many countries, as Unz observes?
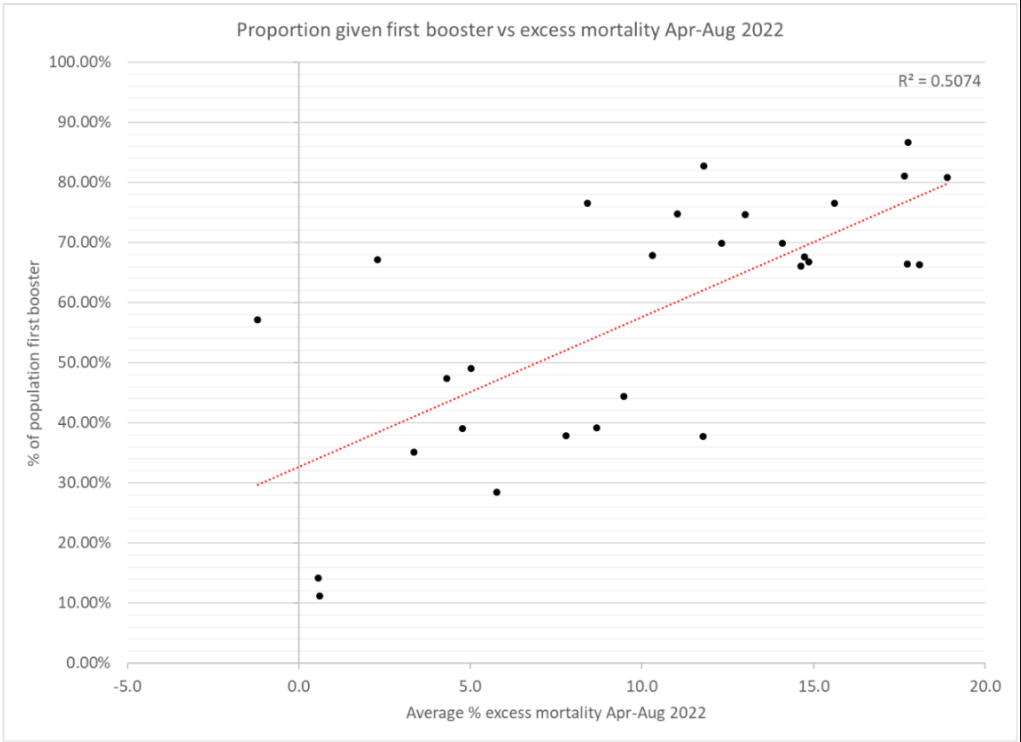
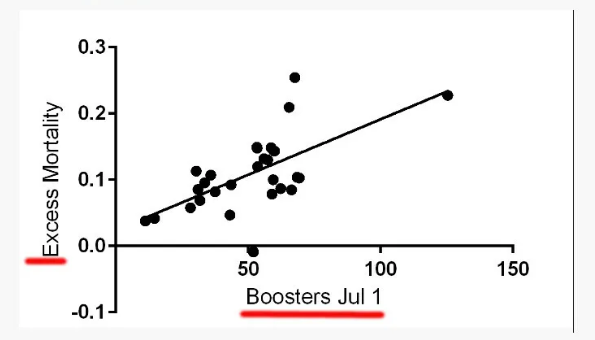
Differences in vaccination rates may be doing their bit here. Some analyses have suggested that higher booster rates are associated with higher deaths in 2022.
So, this may explain some of the variation. Also, recall that for working-age mortality, Unz’s analysis shows that one of the main predictors of 2022 mortality is 2020 mortality, suggesting a common cause in both years. A natural interpretation of this, given the drop in Covid severity and the arrival of the vaccines, is that populations less susceptible to COVID-19 are, for the same reasons – such as prevalence of obesity, heart disease and so on – also less susceptible to fatal vaccine injury.
What we really need, of course, are more and better data – split by vaccination status, age, health conditions, prior infection status and so on. Even better, we need well-designed, prospective controlled studies that look into these things properly. The fact that, after more than two years, we still have none of these things should give even the most ardent defenders of the vaccines pause for thought. If the data were favourable to the vaccines, would they not have been made available with great fanfare long ago?
In the meantime, it’s clear that the vaccines are still a leading suspect in the question of why so many people have been dying, mainly from heart-related issues, in the last two years.