My doctor told me I should get the flu vaccine because the flu can kill people and by taking the vaccine, it will reduce your risk of death. That sounded compelling to me, so I always took the shot when offered.
I now realize that was a big mistake. I regret the error.
To solidify the point, I did a Twitter post recently asking if there was any evidence that anyone should get the flu vaccine.
There wasn’t anything compelling that came back showing I should get the flu vaccine. Are you surprised?
Instead, what I did get back was a lot of compelling evidence that would dissuade anyone from getting the flu vaccine. I think you’ll find the list very interesting!
The bottom line is you should never get any vaccine without first seeing the all-cause risk benefit data.
I rarely go to the @CDCgov Twitter account, but I checked it out today just to see the latest misinformation they are spreading. I’ve found it actually educational since you can often do extremely well by listening to what they advise and doing the opposite.
Here’s the most recent tweet:
So in other words, your risk of flu is now near zero, so plan right now to get a flu shot this fall. I wasn’t able to find the risk/benefit calculation for some reason. Still working on that.
So I posted this:
Here is the study referenced in the tweet which admitted that for over 50 years, there were no studies showing the flu vaccine worked for healthcare workers.
From my Medicare article, check out this chart:
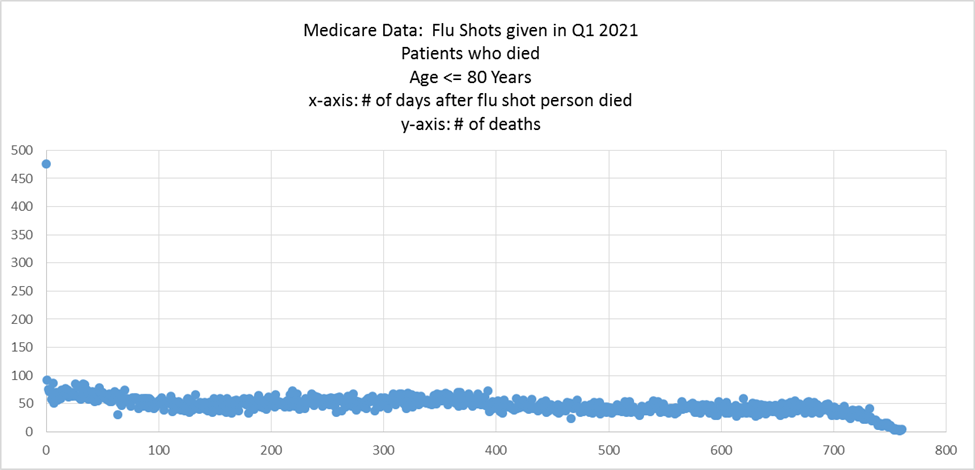
See the 475 deaths on day 0 of the flu shot? That’s impossible for a safe vaccine. It kills around 10 people per million which is 10X higher than what a safe vaccine is supposed to do. This is why the CDC doesn’t let anyone see the Medicare records. They keep them under lock and key.
So basically, there are the risks the CDC never tells you about. Is there a death benefit? No death benefit has ever been established.
So we’re pretty much done right there. No need to read further. But there’s more…
The responses I received on Twitter were also very enlightening.
My favorite response was from James Lyons-Weiler who pointed me to this study: Increased risk of noninfluenza respiratory virus infections associated with receipt of inactivated influenza vaccine which showed the flu vax makes you over 4X more likely to get infected with a non-influenza virus. The result is highly statistically significant. Isn’t that interesting? It reminds me of the COVID vaccine where they looked only at the change in COVID infections instead of looking at the change in anything else (like cancers, heart attacks, death, etc).
Did your doctor warn you about that???
Nobody provided any proof that flu vaccines worked.
There was one person claiming proof, but this does not use a DB RCT. It’s a correlation only. The Turtles book does an awesome job of explaining why this is flawed in their chapter on epidemiology. Basically, to show causality, you need to have a mechanism (which we do) and repeated correlations such as in different countries. The book is great because it gives excellent examples on how epidemiologists are not fooled by a single example like this one.
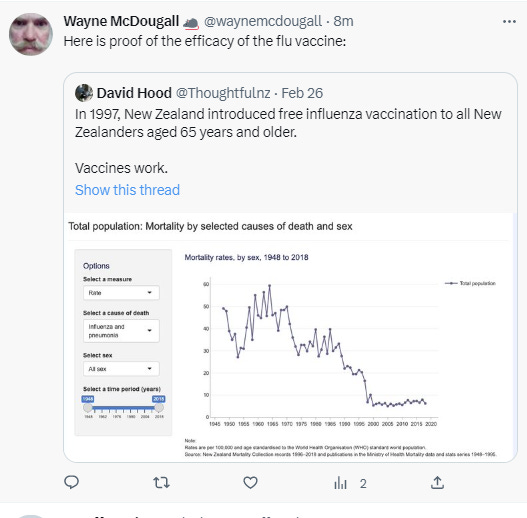
So to show causation, it would have to be repeated in other countries at a minimum. But that isn’t the case as shown in the Our World In Data article.
I bet you cannot tell from the graph below which year they introduced the flu vaccine in the US. And that’s exactly the point.

My second favorite response was from Professor Norman Fenton who linked his video showing the vaccine trick that no health authority will dare explain. In his short video, he shows how the US and UK governments can make a vaccine with 0% efficacy appear to have an efficacy of 86% (2 week delay) or 94.4% efficacy (3 week wait for the vaccine to become effective). Did you realize this?
My third favorite linked to the Cochrane review of the flu for older adults saying the infection risk reduction benefit of 58% was based on low-quality evidence and there was basically no reliable data on a hospitalization or mortality benefit. They wrote:
The study providing data for mortality and pneumonia was underpowered to detect differences in these outcomes.
In short, my doctor did not convey accurate information to me at all.
Then there was the Our World in Data page on the flu which said:
The total number of deaths from influenza has been roughly stable in the United States over the last 65 years.
Then there was the Peter Doshi article saying the same thing I’m saying:
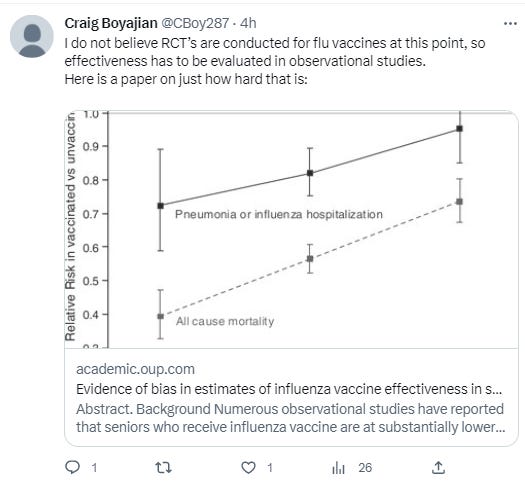
And there was another paper showing that there is a huge discrepancy in the health of the vaccinated and unvaccinated population such that any benefit of vaccination cannot be reliably measured. In fact, if you look at the diagram, the unvaxxed got the exact same relative risk reduction during flu seasons as the vaxxed!!! This is really stunning because the slopes are similar. In other words, whether you were vaxxed or unvaxxed, you got about the same relative benefit (it’s all seasonality) which is why observational studies can’t see the signal; you need DB RCTs which nobody is doing!
Here are some of the other excellent responses:




Flu infections in Australia have been steadily increasing!

The real prophylactic treatment for influenza is NAC. It massively protects from symptomatic influenza episodes.
See this clinical trial:
“The objective of the present study was to evaluate the effect of long-term treatment with NAC on influenza and influenza-like episodes. A total of 262 subjects of both sexes (78% > or = 65 yrs, and 62% suffering from nonrespiratory chronic degenerative diseases) were enrolled in a randomized, double-blind trial involving 20 Italian Centres. They were randomized to receive either placebo or NAC tablets (600 mg) twice daily for 6 months. Patients suffering from chronic respiratory diseases were not eligible, to avoid possible confounding by an effect of NAC on respiratory symptoms. NAC treatment was well tolerated and resulted in a significant decrease in the frequency of influenza-like episodes, severity, and length of time confined to bed. Both local and systemic symptoms were sharply and significantly reduced in the NAC group. Frequency of seroconversion towards A/H1N1 Singapore 6/86 influenza virus was similar in the two groups, but only 25% of virus-infected subjects under NAC treatment developed a symptomatic form, versus 79% in the placebo group. Evaluation of cell-mediated immunity showed a progressive, significant shift from anergy to normoergy following NAC treatment. Administration of N-acetylcysteine during the winter, thus, appears to provide a significant attenuation of influenza and influenza-like episodes, especially in elderly high-risk individuals. N-acetylcysteine did not prevent A/H1N1 virus influenza infection but significantly reduced the incidence of clinically apparent disease.”
De Flora S, Grassi C, Carati L. Attenuation of influenza-like symptomatology and improvement of cell-mediated immunity with long-term N-acetylcysteine treatment. Eur Respir J. 1997 Jul;10(7):1535-41.
There is no clear mortality benefit. There may be an infection benefit, but that seems unlikely.
You need a DB RCT to see the benefits.
There is a reason they don’t do the DB RCTs to prove the vaccine works. Can you guess what it is? Could it be because they don’t want to expose the fact that the vaccines don’t work.
Of course, today they can argue that they are not allowed to test whether the vaccine works or not because they can’t have a true placebo group because it would not be the standard of care.
Convenient, isn’t it?
So based on the rules, we’ll never be able to use a DB RCT to determine whether the vaccine works or not. They like it that way. No complaints from the drug companies on that one!
The best piece of advice I can offer is always demand to see the all-cause risk benefit data before you consent to getting a vaccine, any vaccine. Note: This has never been done for any vaccine.